- Research
- Open access
- Published:
Role of micro-RNAs 21, 124 and other novel biomarkers in distinguishing between group 1 WHO pulmonary hypertension and group 2, 3 WHO pulmonary hypertension
The Egyptian Heart Journal volume 75, Article number: 76 (2023)
Abstract
Background
Pulmonary hypertension “PH” is considered a serious cardiovascular disease. World Health Organization divided PH into groups depending on many factors like pathological, hemodynamic, and clinical pictures. Lately, various micro-RNAs “miRNAs” and other novel biomarkers like endoglin and asymmetric dimethylarginine “ADMA” might have a role in diagnosis of PH and may differentiate between pulmonary arterial hypertension “PAH” and non-PAH. The purpose of the study is to show the role of miR-21, miR-124, endoglin and ADMA in the diagnosis of PH and distinguishing between WHO group 1 PH and WHO group 2 and 3 PH and to identify patients who might benefit from non-invasive and inexpensive tools to diagnose PAH.
Results
miR-21 was upregulated in group 1 PH, and there was significant difference between group 1 PH as compared with group 2 PH, group 3 PH and control; miR-124 was down-regulated in group 1 PH with highly significant difference between group 1 and group 2 PH and control but no significant difference with group 3 PH, endoglin was elevated in group 1 PH with a significant difference as compared to group 2 PH, group 3 PH and control. ADMA was elevated in group 1 PH as compared to control; however, there was no significant difference between it and group 2, 3 PH.
Conclusions
miR-21, miR-124, endoglin and ADMA are good biomarkers to diagnose PH; however, only miR-21 and endoglin could distinguish group 1 PH from group 2 and 3 PH.
Background
Pulmonary hypertension “PH” is considered a serious cardiovascular disease. World Health Organization “WHO” divided PH into groups depending on many factors like pathological, hemodynamic and clinical pictures [1]]. PH is now managed with better diagnostic and treatment tools as compared with the past [2, 3].
Group 1 PH is diagnosed as a mean pulmonary artery pressure “mPAP” ≥ 20 mmhg at rest with pulmonary capillary wedge pressure “PCWP” ≤ 15 mmHg and pulmonary vascular pressure “PVR” > 2 Wood units “WU” [4].
Left heart diseases are one of the most causes of group 2 PH [5]. It is diagnosed as a PAPm of ≥ 20 mm Hg plus a PCWP or left ventricular end-diastolic pressure “LVEDP” ≥ 15 mm Hg. The commonest causes of group 3 PH are chronic obstructive pulmonary disease “COPD,” interstitial lung disease “ILD” and obstructive apnea. The incidence of PH in COPD and ILD is high and reach more than 50% in some studies [6].
One of the most challenging issues is the distinguishing between group 1 PH and other groups especially group 3 PH especially when there are no specific changes differentiating group 1 PH from other forms of PH. Diagnosis of group 1 PH may be strongly accepted if PAH is caused by a known mutation or there is a strong family history of group 1 PH; otherwise, expensive diagnostic tools might be needed to diagnose group 1 PH. So, there is a need for biomarkers allowing differentiating between group 1 PH and PH due to other causes especially chronic lung disease. [7].
MiRNAs have been used recently as markers that can be used for diagnosis and follow-up of the PH progress [8]. The gene expression was regulated negatively by the intracellularly miRNAs across the transcriptome by involvement of specific nucleic acid sequences which leads protein translation inhibition. The pathogenic consequences in PH are affected by the dynamic alteration in their expression, and so might be of diagnostic or prognostic role [9]. MiRNAs can affect several biological processes like cell survival, proliferation and differentiation [10].
ADMA and endoglin help in the diagnosis of PH. ADMA is a natural amino which inhibits the production of nitric oxide “NO.” The release of NO is decreased by the high concentration of ADMA which affects the pathway of NO/cGMP, and this will lead to increase in vascular tone. [11]. ADMA plasma levels might be helpful in monitoring the PAH treatment [12].
Endoglin which was assumed to regulate angiogenesis is considered an important biomarker for diagnosis of patients with PAH and its expression in microvascular endothelium was significantly enhanced [13].
Purpose of the study
-
To assess the role of miR-21, miR-124, endoglin and ADMA in the diagnosis of PH.
-
To develop non-invasive and inexpensive tools that can distinguish between group1 WHO from PH secondary to left sided heart disease “group 2 WHO PH” or lung diseases “group 3 WHO PH.”
Methods
Eighty-eight subjects were included in the study. They were enrolled from cardiology clinic of medical services unit at National Research Center and pulmonary vascular disease unit in chest hospital of Cairo University.
The subjects were divided into 4 groups:
-
1.
30 patients diagnosed with group 1 PH with age range from 20 to 62 years, 10 males, 20 females
-
2.
20 patients diagnosed with group 2 PH with age range from 36 to 67 years, 11 males, 9 females
-
3.
18 patients diagnosed with group 3 PH with age range from 32 to 69 years, 12 males, 6 females
-
4.
20 patients apparently healthy volunteers as controls with age range from 22 to 60 years, 10 males, 10 females
All patients were documented to have PH by right heart catheterization for group 1 PH and other non-invasive tools (echocardiography, chest X ray and CT chest) for group 2, 3 PH. We excluded patients with group 4 and 5 PH, patients with uncertain diagnosis, patients with end stage PH, patients with malignancy or any other systemic diseases.
All the studied groups were subjected to:
-
1.
Full medical history taking with special emphasis on symptoms of PH, drug intake and family history of PH.
-
2.
Full clinical examination including cardiac and chest examination
-
3.
Right heart catheterization
RHC was done to diagnose patients with group 1 PH. A pulmonary artery catheter was introduced to the superior vena cava, right atrium, right ventricle, and PA by qualified operators with patients in the supine position after proper catheter calibration. Pressure waveforms from the RA, PA, and PCWP positions were measured at end expiration. Group 1 PH was diagnosed as a PAPm ≥ 20, PCWP ≤ 15 mmHg and a PVR >3 Wood units in the absence of other causes of precapillary PH like lung diseases, CTEPH.
-
4.
Transthoracic echocardiography
TTE by using Acuson Siemens machine was performed in the left lateral decubitus position in all patients.
Left side assessment included:
-
LV, LA dimensions and functions.
-
Regional wall motions.
-
Valvular lesions.
-
Congenital abnormalities.
Right sided assessment included:
-
RV, RA dimensions and functions.
-
TV velocity and right ventricle systolic pressure (RVSP).
-
Inferior vena cava (IVC) diameter and collapsibility.
-
-
5.
Chest X ray:
Plain chest X ray was done as a work up to diagnose of type 3 PH
-
6.
CT chest:
Non-contrast high resolution CT chest was done as a work up to diagnose group 3 PH.
-
7.
Laboratory tests
A blood sample “5 mL” was taken from each subject then divided, processed and stored according to protocol of each test.
Enzyme-linked immunosorbent assay was used to measure ADMA, endoglin levels after applying the instructions on kits purchased from Elabscience “California, USA catalog No. E-EL-0042.” USA.
Enzyme-linked immunosorbent assay after following instructions on kits purchased from catalog No. E-EL-H 6010 United States.
MiRNAs were extracted from plasma according to the serum/plasma miRNeasy kit protocol, catalog number: 217,184 “Qiagen, Hilden, Germany.” All isolated miRNA were quantified using NanoDrop 1000 “Nanodrop, Wilmington, Delaware, USA.” After the extraction of miRNA, cDNA synthesis was performed using miScript II Reverse Transcription Kit “Qiagen, Germany; catalog number: 218161” by adding 4 µl of miScript HiSpec buffer with 2 µl of 10x miScript Nucleics Mix, 7 ul of nuclease free water, 2 ul of miScript II Reverse Transcription mix and 5 ul of the isolated miRNA. The resulting double-stranded “ds” cDNA was a template for an in vitro transcription “IVT” reaction by using SYBER Green PCR Kit “catalog No. 218073”, by adding 12.5 ul master mix, 2.5 ul universal primer, 2.5 ul primer assay, 4.5 ul nuclease free water and 3 ul of cDNA.
Real-time Quantitative PCR was performed using Rotor gene Q Real Time PCR System “Qiagen, Valencia, CA, USA.” The relative expression levels of miR-21, miR-124 were calculated and normalized to miR-16 “Applied Biosystems, Foster City, CA” using 2−ΔΔct method [14]. MiR-16 was used as a standard miRNA to compare expression levels of other miRNAs in serum. The CT is defined as the PCR cycle at which the fluorescent signal of the reporter dye crosses an arbitrarily placed threshold [15].
Statistical analysis
SPSS version 18.0 for Windows from SPSS, Inc. “IL, USA” was used for data entry and analysis. Qualitative data that presented by numbers and percentages were assessed by using Chi square. Continuous data were expressed as mean and standard deviation. We compare between two means by using t-test and more than two means were assessed by using ANOVA. Two or more independent samples were compared by using Kruskal–Wallis tests when the data are not normally distributed.
Receiver-operating characteristic “ROC” analysis was used to obtain the area under the curve “AUC” and the corresponding 95% CI. The maximum cutoff point was measured which corresponds to the highest Youden index for each biomarker. The AUC for each significant biomarker was assessed by using the ROC curve. The sensitivity, specificity, positive predictive values “PPV” and negative predictive values “NPV” were calculated for the identified cutoff points for each biomarker. P value < 0.05 is considered significant, and < 0.01 is considered highly significant.
Results
Thirty patients with group 1 PH, 20 patients with group 2 PH and 18 patients with group 3 PH were included in the study. 20 apparently healthy volunteers as control group were also included in the study.
-
The results showed no significant difference between the 3 groups of patients and the controls as regards age, sex and Body mass index “BMI” (Table 1)
Table 1 Comparison between the 3 groups of PH and controls regarding age, sex and BMI -
Plasma expression of miR-21 was significantly higher among patients with group 1 PH compared to patients with group 2 and group 3 PH and controls, no significant difference between group 2 PH, group 3 PH and controls, which indicates that miR-21 could be a reliable biomarker differentiating group 1 PH from other 2 groups of PH. As regards plasma expression of MiR-124, it was lower in group 1 PH patients and group 3 PH patients as compared to group 2 PH patients and controls, indicating the value of miR-124 to differentiate group 1 PH from group 2 PH and control. Both miRNAs could be used as diagnostic biomarkers for group 1 PH (Table 2, Figs. 1, 2).
Table 2 Comparison between the studied groups regarding miR-21 and miR-124 expression Fig. 1 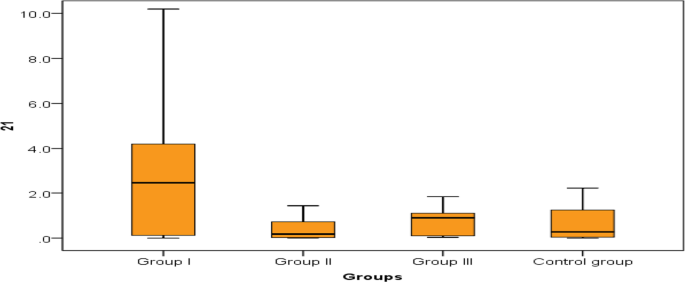
Comparison between the studied groups regarding miR-21
Fig. 2 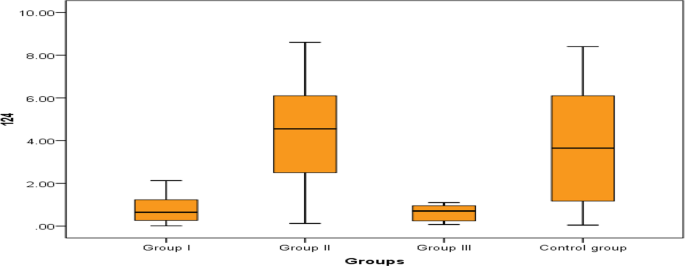
Comparison between the studied groups regarding miR-124
-
Regarding the potential value of ADMA and endoglin to differentiate between group 1 PH and group 2, 3 PH and control, we found no significant difference as regard serum ADMA levels between the 3 groups of the patients; however, it was significantly elevated in group 1, 2 and 3 PH patients as compared to controls which indicate that ADMA could be helpful in the diagnosis of PH in general but couldn't differentiate between the PH groups. On the other hand, serum endoglin levels were significantly higher in group 1 PH compared to group 2 and group 3 PH and to controls (Table 3, Figs. 3, 4).
Table 3 Comparison between the studied groups regarding ADMA and endoglin Fig. 3 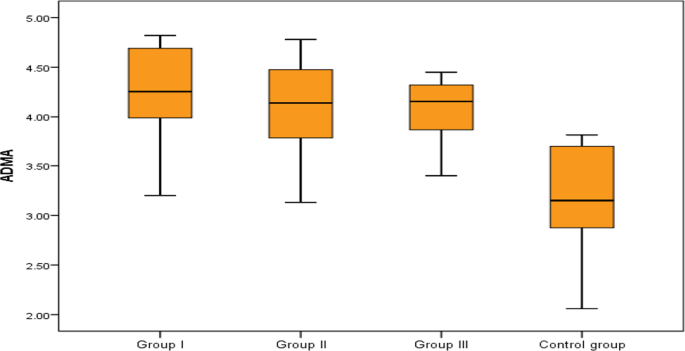
Comparison between the studied groups regarding ADMA
Fig. 4 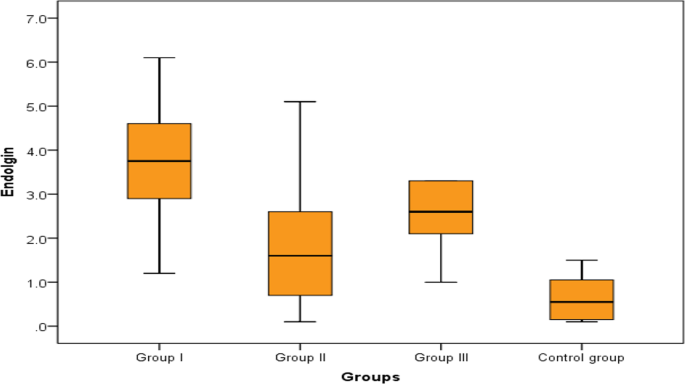
Comparison between the studied groups regarding endoglin
-
To assess predictive value of miR-21, miR-124 and endoglin in the diagnosis of group 1 PH constructed, we constructed ROC curve. We found that the cut off predictive value of miR-21 was ≥ 1.55 µM with 60% sensitivity, 95% specificity with AUC (0.742). The cut off predictive value of miR-124 was ≤ 1.58 µM with 86.7% sensitivity, 75% specificity with AUC (0.789). As regard endolgin, the cut off predictive value was ≥ 1.5 ng/ml with 93.3% sensitivity, and 95% specificity with AUC (0.94) (Table 4 , figures 5, 6).
Table 4 Predictive value of miR-21, miR-124 and endoglin for type 1 PH Fig. 5 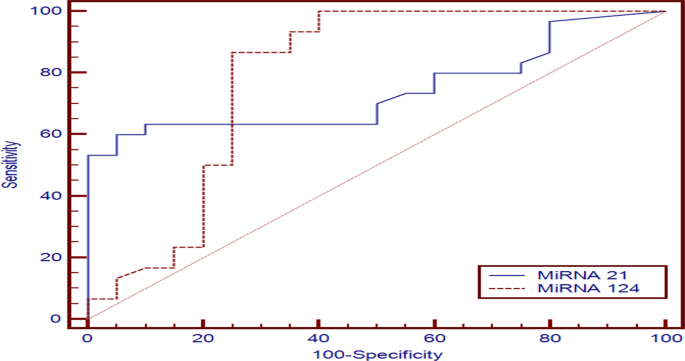
Predictive value of miR-21, miR-124 in group 1 PH
Fig. 6 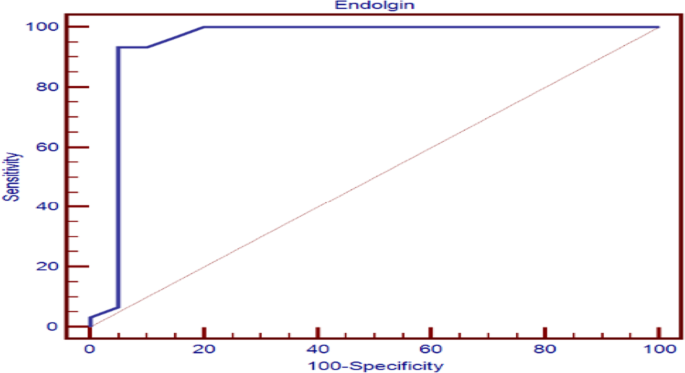
Predictive value of endoglin in group 1 PH






Discussion
There are no specific early signs in PH. The most common symptom is dyspnea especially on exertion; however, it is usually neglected till progression of disease happens with more symptoms developed like chest pain or syncope. As a result of that, PH symptoms deteriorate till diagnosis with delay over 2.8 years [16]. After diagnosis of PH, more than 75% of PH patients have advanced symptoms with complications like pulmonary vascular remodeling and right ventricular failure. Till now, the best available tool in diagnosis of PH is right heart catheterization “RHC.” But because it is an invasive tool so developing new non-invasive diagnostic tools like biomarkers might be important to avoid complications and the high cost of RHC [17].
Unfortunately, the available biomarkers used nowadays for diagnosis of PH are not specific and can be of diagnostic value in late stages of the disease, and they might be also affected by other metabolic functions. However, various biomarkers especially miRNAs are now developed and emerged as a good biomarkers in PH [18].
Our study found that miR-21 was significantly upregulated in patients with group 1 PH and when we compared miR-21 in group 1 PH with group 2, 3 PH and control, we found that there is a highly significant difference between group 1 and group 2 (P = 0.005) and between group 1 and control (P = 0.004) and a significant difference between group 1 and group 3 (P = 0.043). Also, we found that the cut off predictive value of miRNA 21 (≥ 1.55 µM ) has sensitivity (60%), specificity (95%), positive predictive value (94.7%) and negative predictive value (61.3%) with AUC (0.742). So, miR-21 might be used as a good biomarker to differentiate group 1 PH from group 2 and 3 PH.
Upregulation of miR-21 in patients with PAH is affected by hypoxia where HPASMCs had a 3-fold rise in miR-21 level. Bone morphogenic protein 2 “BMPR2” signaling leads to upregulation of miR-21. RhoB is targeted directly by miR-21, and this leads to suppression of its expression and activation of kinase which leads to endothelial dysfunction, inflammation and development of PH [19].
Also, Victoria et al. found that miR-21 integrates multiple pathogenic signals to regulate PH. Hypoxia, inflammation and BMPR2-dependent signaling upregulate miR-21 in the pulmonary vasculature, and this leads to Rho-kinase activation which modulates the development of PH in vivo [20].
Regarding miRNA-124, our study found that miR-124 was down-regulated in patients with group 1 PH and when comparing miR-124 level in group 1 PH with group 2, 3 PH and control, we found that there was highly significant difference between group 1 as compared to group 2 and control (P < 0.001) but no significant difference between group 1 and 3 group. The cutoff predictive value of miRNA 124 (≤ 1.58 µM) has sensitivity (86.7%), specificity (75%), positive predictive value (83.9%) and negative predictive value (78.9%) with AUC (0.789).
Decreased expression of miR-124 modulates fibroblasts phenotype of pulmonary artery, smooth muscle cells “SMCs” and endothelial cells outgrowth from pulmonary hypertensive patients and also miR-124 add-back reversed of these cell's phenotype [21].
Cell proliferation and PH were affected by different factors as the nuclear factor of activated T cells “NFAT” signaling pathway. NFAT activity is inhibited by miR-124 and leads to affection of dephosphorylation, nuclear translocation and NFAT-dependent transcription of IL-2 which shows the beneficial value of miR-124 in preventing PH. Also NFAT pathway was modulated by miR-124 through targeting nuclear factor of activated T cell cytoplasmic 1 “NFATc1,” calmodulin-binding transcription activator 1 “CAMTA1” and polypyrimidine tract-binding protein 1 “PTBP1.” Also, down-regulation of miR-124 in PASMCs and mice lungs was induced by hypoxia so PASMCs proliferation was inhibited by over expression of miR-124 [22].
Transcriptional products from miR-124 genes were examined by Hui Zhang et al., and he reported that PH patients have reduction in the transcription activity of miR-124 gene and that there is epigenetic changes happened due decreased miR-124 expression with the development of PH [23].
Zhang et al. found that miR-124 in patients with PAH was significantly down-regulated with down expression in PASMCs. Also, reduced miR-124 levels in patients with PAH and experimental PH models led to upregulation of polypyrimidine tract–binding protein 1 “PTBP1” by a high proliferative and migratory phenotype. [24].
One of the molecules of the family of transforming growth factor “TGF-β” is endoglin which is a membrane co-receptor. It is involved in vascular development, homeostasis, repair and disease and predominantly expressed by endothelial cells [25].
In our study, we found that expression of endoglin was increased in patients with group 1 PH with a highly significant difference between group 1 PH as compared to group 2 PH and control (P < 0.001) and a significant difference between group and group 3 PH (P = 0.011). Also, we found that a cutoff predictive value endoglin (≥ 1.5 ng/ml) has 93.3% sensitivity, 95% specificity, 96.6% positive predictive value and 90.5% negative predictive value with AUC (0.94), so endoglin might be used as a good biomarker for early diagnosis of group 1 PH and also to differentiate group 1 PH from group 2 and 3 PH.
There is high expression of endoglin in PAH lungs especially in the microvascular endothelial as compared to the lungs of control, and the intensity of expression was more in the sites of dysregulated angiogenesis called plexiform lesion in PAH. The increased concentration of endoglin in blood leads to endothelial dysfunction and proliferation. Endoglin is released from the sites of active remodeling by activation of activation of matrix metalloproteinase-14 “MMP-14” [13]. Expression of endoglin on vesicular endothelial cells is considered as an ancillary receptors for many super family ligand TGF as BMPR2 and serve as to modulate both BMPR2 and TGF-lysical association with activin like kinase receptor 1 “ACTLR-1” gene product [26]. Increased level of endoglin and the occurrence of PAH were due to highly oxidative stress in hereditary hemorrhagic telangiectasia [27]. Endoglin regulates activation and vasomotor tone of endothelial nitric oxide synthase “NOS” through binding with it [28].
In a study performed by Mohammed Noori Al-Dujaili et al., he reported that when comparing PAH patients with healthy subjects regarding endoglin levels, there was a significant difference between the 2 groups [29].
Also, the clinical study of Coral et al. found that the endothelial cells enriched high affinity TGF- receptor with upregulation of endoglin which led to vasculopathy in PAH [30].
In our study we found that levels of ADMA were elevated in group 1 PH with a highly significant difference (P < 0.001) between it and control however there was no significant difference between group 1 PH as compared to group 2 and 3 PH so it failed to differentiate between group 1, 2 and 3 PH.
One of the most important endothelium-derived vasoactive substances is NO which has a vital role in regulating vascular homeostasis and local vasomotor tone. Endothelial dysfunction occurred due to deceased levels of NO. NO is synthesized from L-arginine through the action of NOS. ADMA is an endogenous competitive inhibitor of NOS which blocks the action of NOS and considered a novel biomarker in various diseases such as hypercholesterolemia, coronary artery disease [31], peripheral arterial disease [32], chronic heart failure [33] and PH [34].
Inflammation, collagen deposition, oxidative stress and altered lung function were associated with increasing levels of ADMA. Also, there is a direct association between ADMA levels and obstructive lung diseases [35, 36].
In a study done by Juan Liu et al., he reported that elevated ADMA levels are associated with the presence and severity of PAH in connective tissue disease “CTD” patients, and levels of ADMA in the serum might be used as a valuable biomarker for early diagnosis of CTD-PAH patients [37].
Conclusions
-
MiR-21, miR-124, endoglin and ADMA might be used as non-invasive and inexpensive tools to diagnose PH.
-
MiR-21, endoglin are excellent biomarkers that might be used to distinguish group 1 PH from group 2 and 3 PH.
-
Endoglin is an excellent predictor in the early diagnosis of PAH.
Availability of data and materials
Data and material were available in National Research Center and Chest Hospital in Cairo University.
Abbreviations
- PH:
-
Pulmonary hypertension
- miRNAs:
-
MicroRNAs
- ADMA:
-
Asymmetric dimethylarginine
- PAH:
-
Pulmonary arterial hypertension
- PCWP:
-
Pulmonary capillary wedge pressure
- PVR:
-
Pulmonary vascular pressure
- CTEPH:
-
Chronic thromboembolic pulmonary hypertension
- LVEDP:
-
Left ventricular end-diastolic pressure
- RHC:
-
Right heart catheterization
- HPASMCs:
-
Human pulmonary artery smooth muscle cells
- SMCs:
-
Smooth muscle cells
- NO:
-
Nitric oxide
- BMPR2:
-
Bone morphogenic protein 2
- NFAT:
-
Nuclear factor of activated T cells
- NFATc1:
-
Nuclear factor of activated T cell cytoplasmic 1
- CAMTA1:
-
Calmodulin-binding transcription activator 1
- PTBP1:
-
Polypyrimidine tract-binding protein 1
- TGF-β:
-
Transforming growth factor
- MMP-14:
-
Matrix metalloproteinase-14
- ACTLR-1:
-
Activin like kinase receptor 1
- NOS:
-
Nitric oxide synthase
References
Simonneau G, Montani D, Celermajer DS et al (2019) Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J 53:1801913
Galie N, Humbert M, Vachiery JL et al (2016) 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Rev Esp Cardiol (Engl Ed) 69:177
Galie N, Humbert M, Vachiery JL et al (2016) 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J 37:67–119
Price LC, Weatherald J (2023) The new 2022 pulmonary hypertension guidelines: some small steps and some giant leaps forward for evidence-based care. Eur Respir J 61:2202150
Oudiz RJ (2007) Pulmonary hypertension associated with left-sided heart disease. Clin Chest Med 28:233–241
Thabut G, Dauriat G, Stern JB et al (2005) Pulmonary hemodynamics in advanced COPD candidates for lung volume reduction surgery or lung transplantation. Chest 127:1531–1536
Humbert M, Guignabert C, Bonnet S, Dorfmüller P, Klinger JR, Nicolls MR, Olschewski AJ, Pullamsetti SS, Schermuly RT, Stenmark KR et al (2019) Pathology and pathobiology of pulmonary hypertension: state of the art and research perspectives. Eur Respir J 53:1801887
Min PK, Chan SY (2015) The biology of circulating microRNAs in cardiovascular disease. Eur J Clin Investig 45:860–874
Chun HJ, Bonnet S, Chan SY (2016) Translating microRNA biology in pulmonary hypertension: it will take more than “miR” words. Am J Respir Crit Care Med 195:167–178
Van Rooij E, Olson EN (2007) MicroRNAs: powerful new regulators of heart disease and provocative therapeutic targets. J Clin Investig 117:2369–2376
Zhang S, Yang T, Xu X, Wang M, Zhong L, Yang Y, Zhai Z, Xiao F, Wang C (2015) Oxidative stress and nitric oxide signaling related biomarkers in patients with pulmonary hypertension: a case control study. BMC Pulm Med 15:50
Shafran I, Probst V, Campean J et al (2020) The role of asymmetric dimethylarginine (ADMA) in the follow-up of patients with precapillary pulmonary hypertension (PH). Eur Heart J 41(Supplement_2):ehaa946.2303
Malhotra R, Paskin-Flerlage S, Zamanian RT, Zimmerman P, Schmidt JW, Deng DY, Southwood M, Spencer R, Lai CS, Parker W et al (2013) Circulating angiogenic modulatory factors predict survival and functional class in pulmonary arterial hypertension. Pulm Circ 3:369–380
Yuan Z, Luo G, Li X, Chen J, Wu J, Peng Y (2016) PPARc inhibits HMGB1 expression through upregulation of miR-142-3p in vitro and in vivo. Cell Signal 28(3):158–164
Schmittgen TD, Livak KJ (2008) Analyzing real-time PCR data by the comparative C(T) method. Nat Protoc 3(6):1101
Badesch DB, Raskob GE, Elliott CG, Krichman AM, Farber HW, Frost AE, Barst RJ, Benza RL, Liou TG, Turner M et al (2010) Pulmonary arterial hypertension: baseline characteristics from the REVEAL Registry. Chest 137:376–387
Montani D, Gunther S, Dorfmuller P, Perros F, Girerd B, Garcia G, Jais X, Savale L, Artaud-Macari E, Price LC et al (2013) Pulmonary arterial hypertension. Orphanet J Rare Dis 8:97
Di Stefano V, Zaccagnini G, Capogrossi MC, Martelli F (2011) microRNAs as peripheral blood biomarkers of cardiovascular disease. Vasc Pharmacol 55:111–118
Xiaoyi Hu, Wang Q, Zhao H et al (2022) Role of miR-21-5p/FilGAP axis in estradiol alleviating the progression of monocrotaline-induced pulmonary hypertension. Anim Model Exp Med 5(3):217–226
Parikh VN, Jin RC, Rabello S et al (2012) MicroRNA-21 integrates pathogenic signaling to control pulmonary hypertension. Circulation 125:1520–1532
Kang K, Peng X, Zhang X, Wang Y, Zhang L, Gao L, Weng T, Zhang H, Ramchandran R, Raj JU et al (2013) MicroRNA-124 suppresses the transactivation of nuclear factor of activated T cells by targeting multiple genes and inhibits the proliferation of pulmonary artery smooth muscle cells. J Biol Chem 288:25414–25427
Caruso P, Dunmore BJ, Schlosser K, Schoors S, Dos Santos C, Perez-Iratxeta C, Lavoie JR, Zhang H, Long L, Flockton AR et al (2017) Identification of microRNA-124 as a major regulator of enhanced endothelial cell glycolysis in pulmonary arterial hypertension via PTBP1 (polypyrimidine tract binding protein) and pyruvate kinase M2. Circulation 136:2451–2467
Zhang H, Laux A, Stenmark KR et al (2021) Mechanisms contributing to the dysregulation of miRNA-124 in pulmonary hypertension. Int J Mol Sci 22(8):3852
Zhang H, Wang D, Li M (2017) Metabolic and proliferative state of vascular adventitial fibroblasts in pulmonary hypertension is regulated through a microRNA-124/PTBP1 (polypyrimidine tract binding protein 1)/pyruvate kinase muscle axis. Circulation 136:2468–2485
Ruiz-Llorente L, Gallardo-Vara E, Rossi E, Smadja DM, Botella LM, Bernabeu C (2017) Endoglin and alk1 as therapeutic targets for hereditary hemorrhagic telangiectasia. Expert Opin Ther Targets 21:933–947
Blanco FJ, Santibanez JF, Guerrero-Esteo M, Langa C, Vary CPH, Bernabeu C (2005) Interaction and functional interplay between endoglin and ALK-1, two components of the endothelial transforming growth factor receptor complex. J Cell Physiol 204:574–584
Toporsian M, Jerkic M, Zhou YQ, Kabir MG, Yu LX, McIntyre BAS, Davis A, Wang YJ, Stewart DJ, Belik J (2010) Spontaneous adultonset pulmonary arterial hypertension attributable to increased endothelial oxidative stress in a murine model of hereditary hemorrhagic telangiectasia. Arterioscler Thromb Vasc Biol 30:509–517
Gregory AL, Xu G, Sotov V, Letarte M (2014) Review: the enigmatic role of endoglin in the placenta. Placenta 35:93–99
Al-Dujaili MN, Hussein K, Al-Khafaji A et al (2018) Endoglin level in pulmonary arterial hypertension patients and its association with some criteria. J Pharm Sci Res 10:644–651
Coral-Alvarado PX, Garces MF, Caminos JE, Iglesias-Gamarra A, Restrepo JF, Quintana G (2010) Serum endoglin levels in patients suffering from systemic sclerosis and elevated systolic pulmonary arterial pressure. Int J Rheumatol 2010:969383
Böger RH, Maas R, Schulze F, Schwedhelm E (2009) Asymmetric dimethylarginine (ADMA) as a prospective marker of cardiovascular disease and mortality—an update on patient populations with a wide range of cardiovascular risk. Pharmacol Res 60:481–487
Böger RH, Endres HG, Schwedhelm E, Darius H, Atzler D, Lüneburg N et al (2011) Asymmetric dimethylarginine as an independent risk marker for mortality in ambulatory patients with peripheral arterial disease. J Intern Med 269:349–361
Usui M, Matsuoka H, Miyazaki H, Ueda S, Okuda S, Imaizumi T (1998) Increased endogenous nitric oxide synthase inhibitor in patients with congestive heart failure. Life Sci 62:2425–2430
Gorenflo M, Zheng C, Werle E, Fiehn W, Ulmer HE (2001) Plasma levels of asymmetrical dimethyl-L-arginine in patients with congenital heart disease and pulmonary hypertension. J Cardiovasc Pharmacol 37:489–492
Scott JA, North ML, Rafii M, Huang H, Pencharz P, Subbarao P et al (2011) Asymmetric dimethylarginine is increased in asthma. Am J Respir Crit Care Med 184:779–785
Di Gangi IM, Pirillo P, Carraro S, Gucciardi A, Naturale M, Baraldi E et al (2012) Online trapping and enrichment ultra performance liquid chromatography-tandem mass spectrometry method for sensitive measurement of “arginine-asymmetric dimethylarginine cycle” biomarkers in human exhaled breath condensate. Anal Chim Acta 754:67–74
Liu J, Fu Q, Jiang L et al (2019) Clinical value of asymmetrical dimethylarginine detection in patients with connective tissue disease-associated pulmonary arterial hypertension. Cardiol Res Pract 2019:1–8
Acknowledgements
The authors gratefully acknowledge the studied participants for their enrollment in the project.
Funding
National Research Center funded this work through a Project Number: 12060152. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
Author information
Authors and Affiliations
Contributions
MO (funding acquisition) designed the research steps and implementation. MO, YM, RI, HM and FE conducted data collection and were responsible for patients’ selection, performing investigations to patients. SA, EM, RN and EA participated in performing the laboratory work and results collection. MO contributed to the data entry, statistical analysis and tabulation. MO, YM and HM wrote, reviewed and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by ethical committee of National Research Center.
Ethical committee's name: Prof: Samia Temtamy-Head of Medical Research Ethical Committee (MREC).
Date of approval: 2019.
Reference number: 19-288.
All participants were provided an informed written consent to participate in the study in accordance with the code of ethics of the World Medical Association (Declaration of Helsinki) for experiments on humans (all patients were aged above 20 years old)
Consent for publication
Not applicable.
Competing interests
The authors declared that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dimitry, M.O., Soliman, Y.M.A., ElKorashy, R.I. et al. Role of micro-RNAs 21, 124 and other novel biomarkers in distinguishing between group 1 WHO pulmonary hypertension and group 2, 3 WHO pulmonary hypertension. Egypt Heart J 75, 76 (2023). https://doi.org/10.1186/s43044-023-00395-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43044-023-00395-w